Metástasis cerebrales: estadificación y tratamiento
encontrar mi
¿Qué es la estadificación del cáncer?
La estadificación es el proceso de determinar la cantidad de cáncer presente en el cuerpo y su ubicación. Las metástasis cerebrales no se estadifican, pero sí influyen en la etapa del cáncer primario (el lugar donde se originó). Para obtener más detalles sobre la etapa de su cáncer, consulte el artículo sobre estadificación correspondiente a su tipo de cáncer primario.
Si su proveedor cree que puede tener metástasis cerebrales, es posible que solicite estudios de diagnóstico de imágenes, como una resonancia magnética y una tomografía computarizada para mirar su cerebro. Puede que necesites una biopsia si se desconoce el tipo de cáncer primario o si ha pasado mucho tiempo desde su tratamiento para el cáncer primario inicial y sus nuevos síntomas.
Opciones de tratamiento
El tratamiento para las metástasis cerebrales depende de muchos factores, como el estadio primario del cáncer y los tratamientos que esté recibiendo, su edad, su estado general de salud y la cantidad de metástasis cerebrales. Su tratamiento puede incluir algunos o todos los siguientes tratamientos:
- Corticosteroides.
- Cirugía.
- Radioterapia cerebral completa (RTCC).
- Radiocirugía estereotáctica (SRS).
- Quimioterapia.
- Terapia dirigida.
- Inmunoterapia.
- Ensayos clínicos.
Cada cáncer primario actúa y se trata de forma diferente. Las opciones de tratamiento para las metástasis cerebrales dependen del tipo de tumor primario.
Manejo de los síntomas con corticosteroides
El cráneo es duro y protege el cerebro. No hay mucho espacio extra dentro del cráneo. Las metástasis cerebrales ocupan espacio en el cerebro, ejerciendo presión sobre el tejido circundante. Esta presión puede causar síntomas. El primer objetivo del tratamiento es aliviar parte de esta presión disminuyendo la inflamación. Para hacer esto, se utilizan medicamentos llamados corticosteroides (la dexametasona o prednisona). Se pueden administrar por vía oral o a través de un catéter intravenoso (IV, en una vena). Algunas personas se sienten mejor poco después de comenzar el tratamiento con esteroides. Sin embargo, esto no significa que el tumor haya desaparecido. También podrían administrarle medicamentos para tratar o prevenir las convulsiones.
Cirugía
La cirugía puede utilizarse para tratar una metástasis (lesión), especialmente si el cáncer está controlado en el resto del cuerpo. La lesión debe estar en una zona del cerebro donde sea seguro operar. Estudios han demostrado que los pacientes con una sola metástasis cerebral que se sometieron a cirugía seguida de radioterapia cerebral completa (RTCC) presentan menos recurrencias (cuando el cáncer regresa) y una mejor calidad de vida que los pacientes tratados solo con RTCC.
Radioterapia cerebral completa
La radioterapia cerebral completa (RTCC) es radiación administrado a todo el cerebro. RTCC:
- A menudo se administra en 10 a 15 dosis (también llamadas fracciones).
- Se utiliza a menudo cuando la cirugía no es una opción o cuando hay más de 3 metástasis cerebrales.
- La RTCC también se puede utilizar con radiocirugía estereotáctica/SRS (ver a continuación).
Se trata todo el cerebro porque puede haber células cancerosas, pero aún no en cantidades suficientes como para formar una lesión visible en una tomografía computarizada o una resonancia magnética. El tratamiento integral del cerebro busca eliminar todas las células cancerosas, incluso las que aún no se ven.
La radioterapia de tejido conectivo (RTCC) mejora los síntomas de las metástasis cerebrales en muchos pacientes, aunque parte de esto también se debe a los corticosteroides. Las metástasis cerebrales pueden reaparecer. Los pacientes con tumores más sensibles a la radiación tienden a responder mejor (cáncer de pulmón y de mama, por ejemplo) que aquellos con tumores menos sensibles a la radiación (melanoma y cáncer renal).
Radiocirugía estereotáctica (SRS)
Radiocirugía estereotáctica (SRS) no es una cirugía. Es una gran dosis de radiación dirigida al tumor, administrada con mucha precisión. Es necesario mantener la cabeza muy quieta usando un casco o máscara para que no te muevas durante el tratamiento.
La SRS se administra en una sola dosis (Gamma Knife®) o hasta en cinco dosis (Cyberknife®). Se puede tratar más de una metástasis cerebral en una sola sesión. Por ejemplo, si tiene dos metástasis cerebrales, ambas podrían tratarse el mismo día. Los tratamientos se administran mediante un aparato de radiación tradicional llamado acelerador lineal, o con aparatos como Gamma Knife®, Cyberknife®, XKnife® y ExacTrac®.
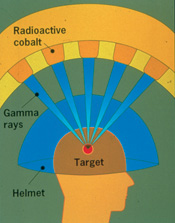
El Gamma Knife® administra cientos de haces de radiación desde una fuente de cobalto. Los haces de radiación se concentran (se unen) en el punto donde se unen todos los haces (ver imagen). Los haces de radiación viajan a través de cientos de orificios en el casco. Esto permite administrar una alta dosis de radiación al tumor, protegiendo al mismo tiempo el tejido circundante.
XKnife® es un tratamiento basado en aceleradores lineales. Al igual que el Gamma Knife, se utiliza un marco para el cabezal que permanece colocado durante todo el tratamiento.
Cyberknife® es una forma de SRS sin marco que utiliza un acelerador lineal miniatura especializado con un brazo robótico. En lugar de usar un marco para mantener al paciente inmóvil, se utiliza una máscara personalizada para cada paciente junto con un sistema de seguimiento basado en el cráneo, lo que permite al robot seguir un objetivo. Cyberknife® también puede tratar lesiones mayores de 3 cm y puede utilizarse en otras partes del cuerpo.
Terapia de protones es una forma más reciente de SRS. Una máquina llamada sincrotrón o ciclotrón acelera los protones y los dirige al tumor. La alta energía de estos protones en movimiento puede destruir las células cancerosas. Durante el tratamiento, los protones pueden dirigirse con precisión al tumor. La terapia de protones se administra generalmente 5 días a la semana durante aproximadamente 4 a 8 semanas. Su equipo de atención médica hablará con usted sobre las mejores opciones de radiación y elaborará un plan de atención basado en su caso.
Quimioterapia
La quimioterapia es el uso de medicamentos contra el cáncer para tratarlo. Se cree que la mayoría de la quimioterapia no pueden entrar al cerebro. Esto se debe a la barrera hematoencefálica. Estos medicamentos pueden viajar por el torrente sanguíneo, pero no pueden llegar al cerebro. Un medicamento de quimioterapia, la temozolomida (Temodar®) es un medicamento oral que atraviesa la barrera hematoencefálica. Puede utilizarse para tratar algunas metástasis cerebrales.
Algunos otros medicamentos pueden llegar al cerebro, especialmente los metástasis cerebrales que provienen de tumores primarios que responden bien a la quimioterapia (como el cáncer testicular, los linfomas y el cáncer de pulmón de células pequeñas).
Terapia dirigida
Estas terapias se dirigen a cambios específicos en una célula que favorecen el crecimiento y la propagación del cáncer. Se analizará su tumor para detectar estos objetivos específicos.
Existen muchas terapias dirigidas para tratar las metástasis cerebrales. Los tipos de terapia utilizados dependerán del tumor primario. Algunas terapias dirigidas son lapatinib, erlotinib, gefitinib, osimertinib, vemurafenib, alectinib, brigatinib, ceritinib, tucatinib, y trastuzumab.
Inmunoterapia
La inmunoterapia utiliza el propio sistema inmunitario del cuerpo para detectar y destruir las células cancerosas. También se denomina terapia biológica. Algunos medicamentos de inmunoterapia que se utilizan para tratar las metástasis cerebrales son ipilimumab, nivolumab y pembrolizumab, dependiendo de la ubicación del tumor primario. La terapia CAR-T también se está estudiando en ensayos clínicos como una opción de tratamiento para las metástasis cerebrales en algunos tipos de cáncer.
Para obtener más información sobre su tipo específico de cáncer y su tratamiento, utilice nuestro tipos de cáncer menú.
Ensayos clínicos
Es posible que le ofrezcan un ensayo clínico como parte de su plan de tratamiento. Para obtener más información sobre los ensayos clínicos actuales, visite Servicio de emparejamiento de ensayos clínicos OncoLink.
Toma de decisiones sobre el tratamiento
Su equipo de atención se asegurará de que usted participe en la elección de su plan de tratamiento. Esto puede ser abrumador, ya que podrían ofrecerle varias opciones. Está bien tomarse un tiempo para reunirse con diferentes proveedores y considerar sus opciones y qué es lo mejor para usted. Esta es una decisión personal. Sus amigos y familiares pueden ayudarle a analizar las opciones y las ventajas y desventajas de cada una, pero no pueden decidir por usted. Debe sentirse cómodo con su decisión; esto le ayudará a avanzar. Si tiene alguna pregunta o inquietud, no dude en llamar a su equipo.