Esófago de Barrett: Un resumen
encontrar mi
¿Qué es el esófago?
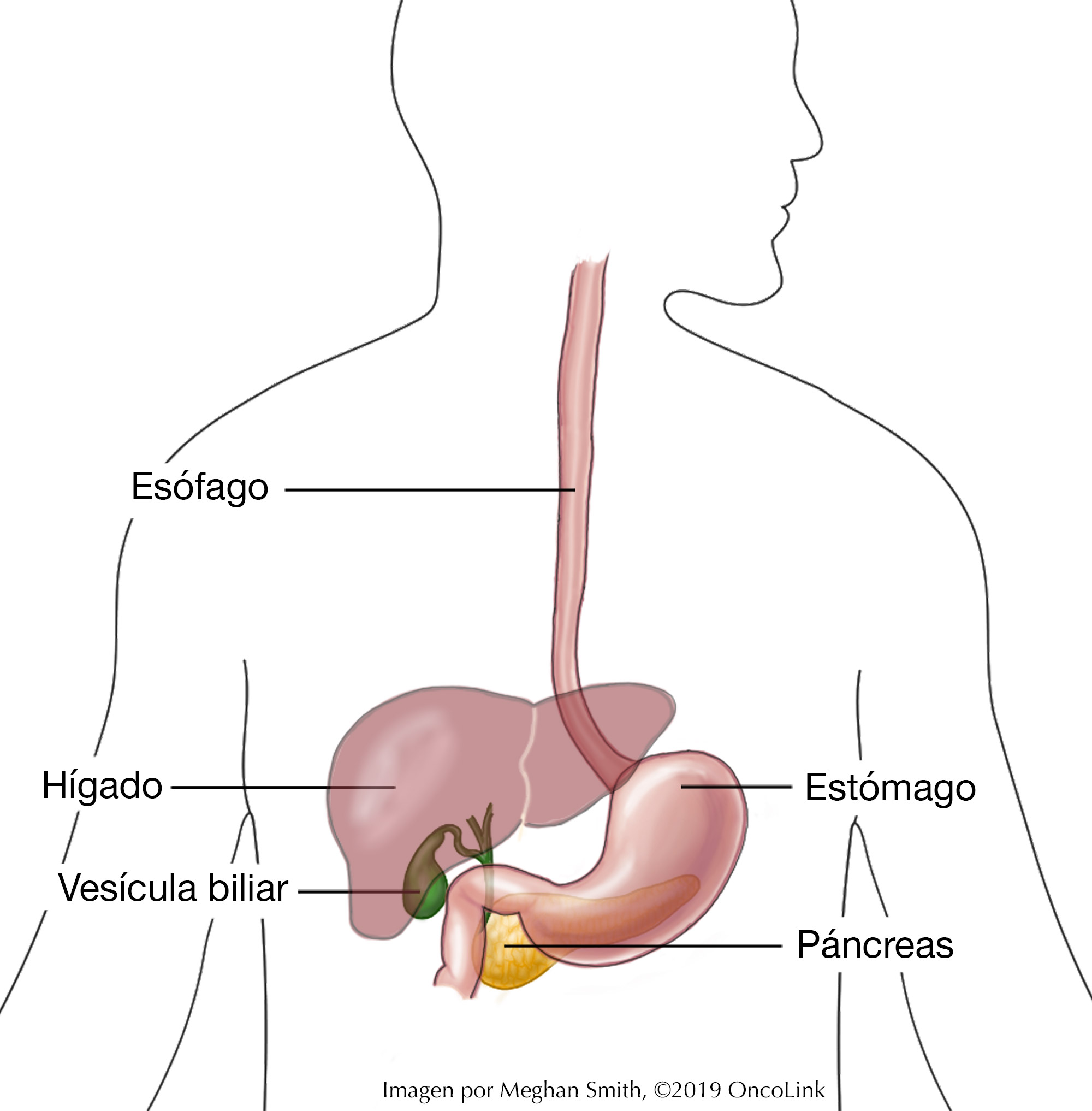
El esófago es un tubo que conecta la garganta con el estómago.
¿Cómo funciona el esófago?
Transporta los alimentos que tragamos desde la boca hasta el estómago, donde pueden ser digeridos. El esófago mide generalmente unos 25 cm (10 pulgadas) de largo y se une al estómago en la unión gastroesofágica (unión GE). En la unión GE hay un músculo circular que envuelve el esófago, llamado esfínter esofágico inferior. Este no es un músculo que podamos controlar por nuestra cuenta. Normalmente, se abre solo para dejar pasar la comida del esófago al estómago o durante el vómito. El músculo del esfínter esofágico inferior impide que los alimentos y el ácido estomacal regresen al esófago.
El revestimiento del esófago se llama mucosa y protege al esófago de cosas que podrían causarle daño, como el ácido estomacal. Las células que forman la mucosa se reemplazan a un ritmo rápido para ayudar a reparar el daño que ocurre durante la alimentación diaria. Las células de la mucosa son células planas que tienen capas (llamadas “epitelio escamoso estratificado”).
¿Qué es el ácido estomacal?
El ácido estomacal ayuda a digerir los alimentos. Pero, también puede causar daños si hay demasiada cantidad o si regresa al esófago.
¿Qué es el esófago de Barrett?
El esófago de Barrett ocurre cuando las células que forman el revestimiento del esófago cambian debido a un daño y no vuelven a crecer normalmente. Este cambio, llamado metaplasia, aumenta el riesgo de cáncer para la persona. En lugar de estar formado por células planas en muchas capas (“epitelio escamoso estratificado”), hay una sola capa de células altas (“epitelio columnar”), que pueden ser precancerosas.
¿Cómo se relaciona el esófago de Barrett con el cáncer de esófago?
Las personas con esófago de Barrett tienen un mayor riesgo de cáncer de esófago que las personas que no lo tienen. El esófago de Barrett aumenta el riesgo de un cáncer llamado adenocarcinoma de esófago. El esófago de Barrett es una enfermedad “premaligna”, lo que significa que, aunque no es cáncer, puede convertirse en cáncer.
Aunque el riesgo general de adenocarcinoma de esófago es bajo, el esófago de Barrett sigue siendo muy importante clínicamente. Esto se debe a que los tratamientos para el síndrome de Barrett son más exitosos que los tratamientos para el cáncer de esófago.
¿Qué causa el esófago de Barrett? ¿Estoy en riesgo?
La causa más común del esófago de Barrett es la enfermedad por reflujo gastroesofágico (ERGE) o acidez estomacal. Cuando una persona tiene ERGE, el ácido estomacal sube hacia el esófago, causando daños repetidos en el revestimiento del esófago. Muchas personas con esófago de Barrett tienen antecedentes de acidez estomacal o regurgitación ácida que duran al menos 10 años. Sin embargo, algunas personas desarrollan esófago de Barrett sin presentar nunca síntomas de reflujo. Algunos de los factores de riesgo conocidos son:
- Tener 50 años o más.
- Antecedentes actuales o familiares de esófago de Barrett.
- Sexo masculino al nacer.
- Raza blanca (caucásica).
- Tener ERGE crónica.
- Hernia hiatal (una afección en la que parte del estómago sobresale hacia el pecho).
- Tener exceso de peso alrededor de la cintura.
Aunque es menos común y menos estudiada, la bulimia con vómitos también puede aumentar el riesgo de esófago de Barrett debido al daño al esófago por vómitos repetidos.
¿Cómo puedo prevenir el esófago de Barrett?
Las formas de prevenir el esófago de Barrett se centran en el tratamiento de la ERGE crónica. Trabaje con su proveedor de cuidado médico para elaborar un plan. Este plan puede incluir:
- Tomar medicamentos antiácidos.
- Dejar de usar productos de tabaco.
- Controlar el peso.
- Comer comidas pequeñas y frecuentes.
- Evitar comer tres horas antes de acostarse.
- Evitar agacharse después de comer.
- Elevar la cabecera de la cama para ayudar a la digestión.
- Evitar alimentos picantes, ricos en grasas, lácteos o ácidos.
¿Qué pruebas de detección hay disponibles?
La Asociación Estadounidense de Gastroenterología no recomienda realizar pruebas de detección del esófago de Barrett a la población general. Se le debe realizar una prueba de detección si tiene síntomas crónicos o frecuentes de ERGE y dos o más factores de riesgo de esófago de Barrett o adenocarcinoma de esófago. Las mujeres tienen un riesgo menor que los hombres de padecer esófago de Barrett. Sin embargo, se puede recomendar la detección a las que tienen factores de riesgo. Los factores de riesgo son los mismos para mujeres y hombres.
No existe evidencia que oriente la detección, y esta es invasiva y costosa. Antes de realizar cualquier prueba, se debe considerar la salud actual y la expectativa de vida del paciente. La detección del esófago de Barrett se puede realizar mediante:
- Endoscopia superior: En este procedimiento, lo sedarán y le colocarán una cámara en un tubo largo y delgado en la boca hasta llegar a su garganta, para que su médico pueda ver dentro de su esófago.
- Endoscopia transnasal sin sedación: En este procedimiento, se introduce un tubo largo y delgado por la nariz y baja por la garganta para observar el esófago.
- Prueba de la cápsula: En esta prueba, se ingiere una cápsula sujeta a un pequeño cordón con una esponja o globo en su interior. Una vez ingerida, la esponja o globo se expande y, al extraerla, recoge muestras de tejido del esófago.
¿Cuáles son los signos de esófago de Barrett?
Los signos de ERGE también pueden ser signos de esófago de Barrett. Los signos de ambos son acidez de estómago, eructos, náuseas, regurgitación, sabor amargo en la boca, malestar abdominal y tos seca.
¿Cómo se diagnostica el esófago de Barrett?
El esófago de Barrett se diagnostica mediante endoscopia superior. La endoscopia superior le permite al médico observar el interior de estos órganos y encontrar úlceras, crecimientos anormales y otras afecciones, como el esófago de Barrett. Durante la endoscopia se toman muchas biopsias. Luego se examina el tejido bajo un microscopio para ver si hay cambios en las células de la mucosa que se parecen al esófago de Barrett. Las biopsias también son importantes para asegurarse de que no haya cáncer presente. Todas las biopsias deben ser examinadas por dos o más patólogos, y al menos uno debe ser un experto en patología del esófago.
¿Cómo se estadifica el esófago de Barrett?
La gravedad del esófago de Barrett se describe de dos maneras:
- Si hay displasia y por el grado.
- La cantidad de enfermedad (medida según los criterios de Praga).
La displasia describe una apariencia anormal de las células bajo el microscopio. Las células más altamente anormales tienen mayor probabilidad de convertirse en cáncer. La displasia puede ser de bajo o alto grado y tiene el siguiente espectro:
- Metaplasia
- Displasia de grado bajo.
- Displasia de grado alto.
- Cáncer invasivo.
Los criterios de Praga C&M son un conjunto de reglas que permiten al equipo de atención determinar la gravedad del esófago de Barrett. Los criterios se describen a continuación:
- “C” es la extensión circunferencial de la enfermedad. Se determina midiendo la distancia desde la unión GE hasta el área más alta donde hay metaplasia alrededor de la circunferencia del esófago.
- “M” es la extensión máxima de la enfermedad. Es la distancia desde la unión GE hasta la zona más alta de metaplasia.
Cuanto más alto sea el número de Praga C&M (por ejemplo, C3 M5), más grave será el esófago de Barrett y mayor el riesgo de cáncer.
¿Cómo se trata el esófago de Barrett?
El tratamiento en personas con esófago de Barrett está dirigido a tratar el reflujo ácido. Esto lo hace a menudo con medicamentos. Sin embargo, también se pueden utilizar métodos quirúrgicos y de erradicación endoscópica.
Medicamentos
Se pueden recetar algunos medicamentos, como inhibidores de la bomba de protones (omeprazol, lansoprazol, pantoprazol, etc.) y bloqueadores de H2 (famotidina). Estos medicamentos actúan reduciendo la cantidad de ácido que se produce en el estómago. Los inhibidores de la bomba de protones suelen ser más eficaces que los bloqueadores de H2. En los últimos años se ha investigado si la aspirina puede reducir el riesgo de adenocarcinoma de esófago. En este momento, no se deben recetar aspirina ni medicamentos no esteroides de forma rutinaria a pacientes con esófago de Barrett, a menos que estén indicados como tratamiento para otra afección médica.
Cirugía
También existen muchas cirugías antirreflujo, como la funduplicatura, que se pueden realizar para controlar el reflujo. El Colegio Estadounidense de Gastroenterología no recomienda la cirugía antirreflujo ni los inhibidores de la bomba de protones en dosis altas para la prevención del adenocarcinoma de esófago, aunque estas terapias pueden y deben utilizarse todavía para tratar los síntomas del reflujo crónico.
En algunos casos, se puede realizar una esofagectomía, en la que se extirpa parte o la totalidad del esófago. Luego se reconstruye el esófago utilizando partes del estómago o del intestino grueso.
Erradicación endoscópica
La erradicación endoscópica (también llamada ablación endoscópica) es el intento de eliminar células anormales y salvar la mayor parte del esófago normal. Este tipo de cirugía utiliza las mismas técnicas que se realizan durante la endoscopia. Se recomienda la erradicación endoscópica en pacientes con displasia de alto grado para intentar eliminar todas las áreas anormales de mucosa. Los pacientes con displasia de bajo grado también pueden ser tratados con erradicación endoscópica, pero también pueden ser seguidos solo con vigilancia endoscópica (un programa establecido de endoscopias para vigilar las células anormales). A menudo, el esófago de Barrett puede reaparecer después de la terapia de erradicación. Su proveedor continuará monitoreándolo con endoscopias según el cronograma recomendado. Hay muchos tipos de erradicación endoscópica.
- La ablación por radiofrecuencia utiliza electricidad y calor para dañar las células y está dirigida a áreas anormales.
- La terapia fotodinámica utiliza una sustancia química llamada fotosensibilizador y una fuente de luz. El fotosensibilizador se coloca en los tejidos o áreas que el médico desea erradicar; cuando la luz se dirige a esas células, la reacción entre la luz y el fotosensibilizador provoca la muerte celular.
- La crioterapia utiliza frío extremo para eliminar las células dañadas.
- La resección mucosa endoscópica para áreas más pequeñas o la disección submucosa endoscópica para áreas más grandes son procedimientos en los que se extrae parte del revestimiento del esófago y se recomiendan si su equipo de atención cree que usted tiene cáncer o precáncer.
Los pacientes que reciben terapia de erradicación acudirán a un centro especializado en el tratamiento del cáncer de esófago y estómago. Este centro podrá realizar cirugía o extirpar el esófago si es necesario.
Ensayos clínicos
Es posible que le ofrezcan un ensayo clínico como parte de su plan de tratamiento. Para obtener más información sobre los ensayos clínicos actuales, visite el sitio del Servicio
de emparejamiento de ensayos clínicos de OncoLink.
Atención de seguimiento
Aunque no es común que el esófago de Barrett provoque cáncer de esófago, aún existe un riesgo, por lo que es importante seguir las sugerencias de su proveedor para el tratamiento y la atención de seguimiento. Asegúrese de seguir las orientaciones de detección y el cronograma que le den para las imágenes si está en riesgo de desarrollar cáncer de esófago.
Este artículo sirve como introducción al esófago de Barrett. Puede encontrar más información sobre el cáncer de esófago y su tratamiento en OncoLink. Debe hablar con su proveedor si le preocupa el esófago de Barrett o el cáncer de esófago.